![]()
I’ve been working as ‘psychophysiologist for hire’ on a project with my LJMU psychology colleague Ruth Ogden. We just published our first paper from this project, together with our collaborators, Chelsea Dobbins (University of Queensland), Jason McIntyre (also LJMU Psychology) and Kate Slade (University of Lancaster). With one thing or another, the paper was in development for a long time, mostly because of the volume of data, but partly because data analyses were quite labour-intensive.
Ruth originally initiated the project and got the funding as part of her ongoing research into time perception. She’d already collected some laboratory data that linked activation of the sympathetic nervous system with a subjective perception that time was passing more quickly than usual. There was already a precedent in the literature for increased body temperature distorting time perception and making it seem as though time was passing quickly. There is also an influential paper that links autonomic activation regulated by the anterior insular cortex with distortions in temporal perception.
The motivation for the current study was to test whether increased sympathetic activation had any influence on temporal perception during everyday life. At this point, enter the ‘psychophysiologist for hire’ with a bunch of wearable sensors to measure electrocardiogram (ECG) and electrodermal activity (EDA).
The design for the study was not complex. Our participants would wear the sensors for six hours on one day and they would be messaged to provide hourly ratings of whether time had passed at a normal rate or more slowly or quickly than usual. Kate Slade did a sterling job running all the logistics behind the data collection, and we ended up with data sets from 67 participants. Looking for any association between our autonomic measures and subjective temporal perceptions while participants were out and about in the world was far from straightforward. We had the issue of physical confounds as people were walking, talking and drinking coffee during the data collection. We also had to deal with a mismatch between our two groups of measures, one of which is measured with high fidelity (1000Hz) and a second subjective measure that is only recorded once an hour.
Our key psychophysiological variables were heart rate and heart rate variability in the form of RMSSD from the ECG. For the EDA, we extracted skin conductance level (SCL) and the frequency of phasic galvanic skin responses (GSR); we differentiated both metrics from the EDA signal using a convex optimisation method. I anticipated that the data would be riddled with artifacts and there would be a lot of ‘bad’ epochs. Therefore, we calculated our psychophysiological variables using a 10s epoch and generated lots and lots of epochs. This was a strategy that allowed us to ‘lose’ a proportion of those epochs and still have enough remaining to represent each hour of data collection. The first step of the psychophysiological data analyses was the usual stuff, filtering and in the case of the heart rate data, interpolation to correct for bad epochs, using an algorithm that we’d already developed from an earlier project.
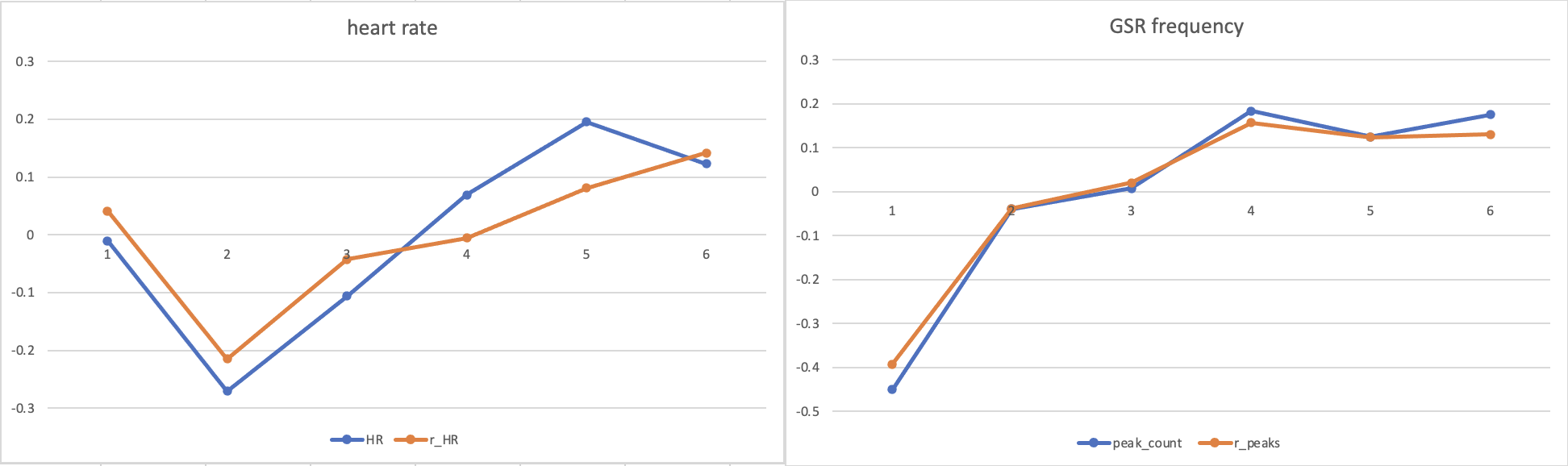
In order to extract the effects of physical activity from our ambulatory psychophysiology, we also had triaxial accelerometers built into our Shimmer ambulatory sensors. First, we created a vector magnitude score that was simply the sum of all movement in 3 possible directions. We know that heart rate increases in the majority of people when they are more active, therefore we used a regression analysis for each participant to model this effect. The residuals from this linear regression, i.e., the proportion of variance in the heart rate signal not explained by changes in physical activity, were standardised and retained for further analysis. EDA is also affected by activity because moving around increases body temperature, which leads to perspiration and a direct influence on the signal. Therefore, because we were expecting the same relationship, increased movement = rises in skin conductance, we did the same regression approach to control for artifacts. The two figures below show the original heart rate and frequency counts of GSR in blue and the residuals retained for analysis in orange. As you can see, the heart rate residual is lower than the original signal in the latter three hours of data collection, which fell in the early afternoon when our participants were most active. By comparison, we didn’t see any noticeable effect of movement on GSR frequency.
The RMSSD was a bit of headache during this study. On one hand, we felt it was important to have an index of parasympathetic activation of the autonomic nervous system. However, as anyone who’s worked with HRV using any of its various metrics knows, it’s very, very susceptible to artifacts. Even one misrecognised R-peak can throw out the whole epoch. So, even after running it through an interpolation algorithm, the RMSSD had to be very carefully checked for outliers and we lost over 18% of the data, which was on the high side. For comparison, we only lost 5% of the EDA data as bad epochs.
The multilevel model used for analyses provided evidence that greater sympathetic activation in the form of increased heart rate and increased frequency of GSR were associated with subjective impression that time was passing more quickly. For clarity, the GSR data is stronger evidence for this conclusion compared to the heart rate data, which is influenced by both branches of the autonomic system, and subject to parasympathetic influence, even though we found no significant influence from RMSSD.
If you’d like to know more, you can read the full paper at the link below:
Ruth also did a short poster presentation about the work at the EPS Conference in 2022. A recording of her talk is below:
{kind=link}