Medical professionals know that distraction is an effective way to distract the patient from a painful procedure, especially when the patient is a child. As a result, there is a lot of work devoted to understanding how technology can distract from pain, particularly using VR in the clinic. The basic idea here is that VR and related technologies have an immersive quality and it is this immersive quality that enables distraction from pain.
When you start to dig into the semantics of immersive technologies, it’s clear that the word is being used in slightly different ways. For VR research, immersion is about creating a convincing illusion of place and an equally convincing version of the body to move through this virtual space. With respect to gaming research, immersion is a graded state of attention experienced by the player of the game. Some games can be played while the player conducts a conversation with someone else, others make more strenuous demands and require total concentration, evoking grunts or monosyllables to any unwelcome attempts at conversations – and a small number of games occupy attention so completely that any attempt to converse will not even be heard by the player.
Moving away from technology, there’s also a load of work in the field of pain research on the relationship between selective attention and pain. According to this perspective, painful sensations call attention to themselves at source, whatever that is, either a hand placed unthinkingly on a hot oven or a foot pierced by a nail. This cry for attention interrupts all other thought processes if the pain is extreme, and so it should from an evolutionary perspective. But the evidence suggests that awareness of painful sensations can be reduced (and tolerance for pain enhanced) by having participants perform cognitive tasks that are very demanding, such as memorising material or doing mental arithmetic. High levels of concentration on a cognitive task makes it harder for painful sensations to call attention to themselves.
So, we see an obvious point of convergence between games and research into pain, namely that painful sensations require attention, which is limited and highly selective, hence we can ‘dampen’ attention to pain by providing the person with an activity that fully occupies their attentional capacity.
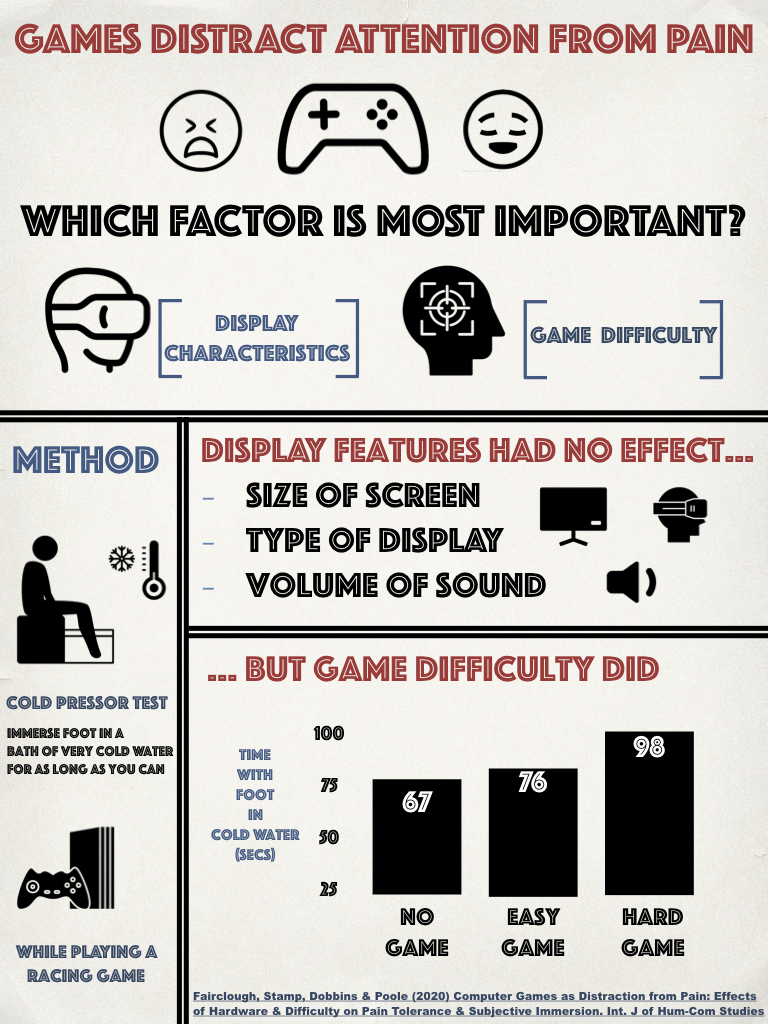
We recently published an experimental paper on the relationship between immersion during gaming and the experience of pain in the International Journal of Human-Computer Studies. The infographic at the top of this post gives a brief study of the work and the four studies included in the paper.
The work was motivated by a desire to understand the influence of two contributions to immersive experiences during games: hardware quality and cognitive demands. Playing a game in VR or on a huge 4K TV screen with surround sound is great of course, but are those kinds of high quality ‘immersive’ displays necessary for distraction from pain? On the flip side of this coin, we have the level of cognitive engagement required to interact with the technology. Engagement can be described as the level of effortful striving required to fulfil the goals of the game. This dimension captures the level of mental and perceptual demands made on the person by the game. In order for a game (any kind of task) to attract selective attention, it is important for the player to engage with the mechanics and the goals of the game.
In the paper, we conducted four studies to understand the influence of hardware and cognition on pain tolerance during game play. We started from the position that highest pain tolerance would be observed when display was immersive and cognitive engagement was high.
In order to induce a modest degree of pain on our participants, we used an experimental protocol called the cold pressor test. The idea behind this method is very simple. The experimenter fills a container with very cold water and the participant must immerse a limb, a foot in our case, in the cold water for as long as they can. If you use very cold water of around 2 degrees centigrade, as we did in all four studies, the subjective experience goes something like this: after the initial shock of the cold water, your limb gets very cold, then it begins to ache while feeling slightly numb, and over a short period, the ache grows worse until you feel compelled to remove your foot from the water. From the perspective of experimental ethics, the cold pressor test works well because the pain is relatively short-lived, the experience remains under the control of the participant and there is no lasting physical damage. The other reason we chose this approach was that the cold pressor test provides a quantitative, behavioural measure of pain tolerance, namely how long participants keep their limb in the water.
The first study in the paper compared pain tolerance using the cold pressor test when 30 participants played a game called InCell with three types of display: a smartphone-based VR display, a TV screen and a head-mounted micro-display that presented a 2D view of the game. InCell was selected for two reasons: (1) at that time, it was one of the few games we could find that was available in VR and 2D form and looked/behaved exactly the same, and (2) it was a racing game with simple controls that required very little training, so even non-gamers could take part. As expected, we found that playing the game increased the time spent with foot immersed in cold water by around 40% (from 30sec to around 48sec), but there was no statistically significant difference between the three display types. The trend was in the expected direction, i.e. 58s for VR vs. 44s for TV, but one drawback with the cold pressor test is that variability between participants can be very high.
In the second study, we turned our focus onto cognitive engagement. I’d already used the futuristic racing game WipeOut HD in an earlier study that utilised evoked cortical potentials to capture gaming immersion. The nice thing about WipeOut (aside from being very easy to learn the controls) that we learned during that study was that the AI setting reliably manipulated the difficulty of the game. So, the difference between ‘Novice’ and ‘Elite’ settings was sufficiently robust that the majority of our participants, regardless of gaming experience, found ‘Novice’ to be reliably easy and ‘Elite’ to be reliably hard. This might sound like an obvious point, but when you’re using commercial software for psychology experiments, getting the settings of the game right is more challenging than you might think. Our 68 participants averaged 52sec during the cold pressor test during a control condition with no game, this figure jumped to 73sec when they played the ‘Novice’ game and increased further to 90sec in the case of the Elite game. By manipulating game demand to increase engagement, we were able to elicit a significant increase of pain tolerance of approx. 29% for an easy game and 43% for a challenging game.
The third study incorporated a simultaneous manipulation of game demand and the size of the screen display. Once again, we used Wipeout with its reliable Novice and Elite settings, but this time, split our 60 participants into two groups; one played the game on a 40″ TV screen and the second played the same game on a 5″ LCD screen. The effect of game demand was similar to the second study, significantly increasing time with limb in cold water by 25% during the Novice setting and 45% for Elite game. But we failed to record any statistically significant effect of screen size on pain tolerance; in fact, the data were not even close to statistical significance.
For the last study, we reverted to the InCell game and conducted the study using the ‘cardboard’ VR display. This fourth study was designed to contrast the effects of sound volume with the influence of game demand on pain tolerance. Sound design makes an important contribution to gaming experience, background music and sound effects are designed to enhance the experience of the game. In this case, we manipulated the demand of the game by varying the speed of the avatar and number of obstacles. To compare the effects of sound volume on pain tolerance, our 40 participants were divided into two groups and exposed to quiet volume setting (11.6dB) to a loud setting (58dB). We reasoned that louder game music and sound effects would make the game more immersive. In this case, the influence of demand on pain tolerance was even more pronounced than the previous three studies, in comparison to a non-game control condition, we saw a 45% increase for the easy game and the foot was left in the cold water for an average of 75% longer when the game was hard. But, no significant effect of game sound volume on pain tolerance was observed.
So, what are we to conclude? First of all, playing a demanding game has a significant effect on pain tolerance. The level of cognitive engagement with the game, as manipulated indirectly by game demand, was a consistent influence on the time recorded during the cold pressor test across three studies, and in general, accounted for approx. 40% of the observed variance. If you look at the full paper (see below), you’ll see we also measured autonomic activation (using heart rate or systolic blood pressure), we found some evidence that autonomic activation: (1) increased with game demand, and (2) directly mediated pain tolerance. So, one of the unanswered questions here is whether pain tolerance increased with game demand largely because of those changes in autonomic activation?
The absence of any strong, significant effects of display characteristics on pain tolerance requires further investigation. We used a limited selection of games and we did not use the highest quality VR experience. But before we rush to bring VR into the pain clinic, perhaps we need a clearer idea about its unique contribution to the known relationship between attention and pain perception.
There are a load of other issues and caveats with the work, which are really best expressed in the paper itself. If you’d like to read the whole thing, the publishers have granted 50 days of free access to the paper (link) that will expire on 5th May 2020.
{kind=link}